Stay safe and confident underwater with expert asthma support.
Home » Asthma and Diving
Quick links:
Asthma is a disease characterized by narrowing of the airways, specifically bronchi, in response to a variety of stimuli (See Image 1.0: Bronchi). It is not a fixed response and a patient can have a sudden worsening in lung function called an “attack.” An asthma attack can be triggered by pollen and other so-called “allergens” such as cold air, irritants in the atmosphere, colds or flu.
Asthma affects over 2 million Australians and as of yet the cause is unknown.
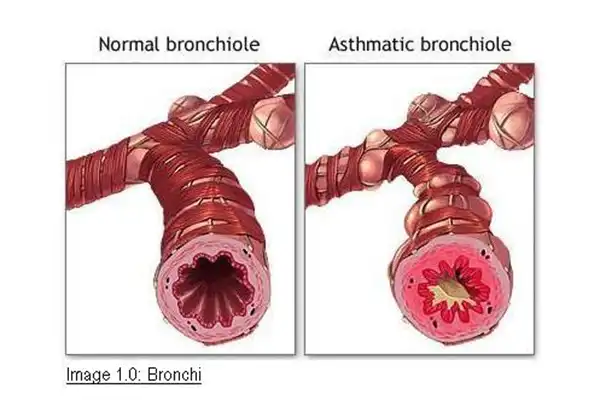
The bronchial narrowing in asthma has two effects: one is to decrease the amount of air that can be moved in and out of the lungs. This can reduce exercise capacity — especially for a diver, who already has reduced breathing capacity due to the external resistance of his breathing apparatus and the increased internal resistance due to higher breathing gas density at depth. Secondly, reduced airway caliber could cause trapping of gas in the lung during ascent.
If trapped gas expands at a rate greater than it can be exhaled through the narrowed airways lung rupture can result, causing arterial gas embolism or pneumothorax (collapsed lung). Another related concern with asthma and diving has been the increased propensity of airways in asthmatics to narrow when exposed to the conditions implicit in diving: inhalation of cold, dry air and/or sea water (the latter by losing the mouthpiece or from a leaky regulator). Dr. Mark Harries from the British Medical Olympic Center has pointed out that asthmatics who dive are at risk from exercise limitation, not just peripheral gas-trapping. While exercising on land it is easy enough to stop, rest and catch one’s breath; this may not be possible underwater.
It is recommended that asthmatics maintain a relationship with their specialist for maintenence of their condition during their diving careers.
There is a high prevalence of asthma in the Australian and New Zealand population.
Strenuous exercise is frequently required of the diver, and there are many opportunities for accidental aspiration of sea water to occur. Inhaling dry air from a tank or fine aerosols of hyperosmolar saline through a faulty valve are stimuli also encountered by the diver. In the last decade there has been a nationwide effort to improve education of doctors and patients about asthma and its treatment through advertising campaigns. Inhaled corticosteroids are more available and more widely used than they were 10 years ago. Lung function tests are more commonly requested and the testing apparatus used in laboratories is more sophisticated, permitting measurements of flow at low lung volumes.
It is now clear that bronchial hyperresponsiveness (BHR) to hyperpnea of dry air, an absolute contraindication for SCUBA diving, can be associated with normal values for resting spirometry.
Currently most laboratories provide a choice of bronchial provocation tests. The role of the bronchial provocation test in the assessment of the diver or intending diver should be to identify those persons who would be at risk from acute airway narrowing during the activities associated with diving.
Those who have demonstrable BHR should be told that they may be at increased risk of pulmonary barotraumas and the details of the possible consequences of this should be explained.
The following questions were asked to people wishing to begin a diving course prior to completing a bronchial provocation test. Subsequently these people were confirmed to have asthma.
The Mannitol challenge is a type of bronchial provocation test. Mannitol is a naturally occurring sugar alcohol which is a stable compound with few side-effects. Following inhalation, Mannitol is deposited on the airway surface which causes an increase in osmolarity of the airway surface liquid. Water then moves out of the epithelial cells in an attempt to restore balance, causing the epithelial cells to shrink. As the cells attempt to regain their volume, intracellular calcium rises, which is thought to trigger the release of inflammatory mediators such as histamines, prostaglandins and leukotrienes. In sensitive individuals the release of these mediators causes the bronchial smooth muscle to contract and the airways to narrow. This is measured by a fall in FEV1 (Forced Expiratory Volume in one second).
Click on any of the links below for more information regarding Asthma and Diving.
Stay informed with expert tips, research updates, and wellness insights from our team of respiratory and sleep medicine professionals.
Blog of the Week

Struggling to stay comfortable while using your CPAP machine? The right pillow can make a
Recent

As the body, the brain and the senses adjust to wearing a CPAP mask, it

Foods that contain melatonin, tryptophan, certain carbohydrates and magnesium are those that aid sleep, but
Struggling to stay comfortable while using your CPAP machine? The right pillow can make a
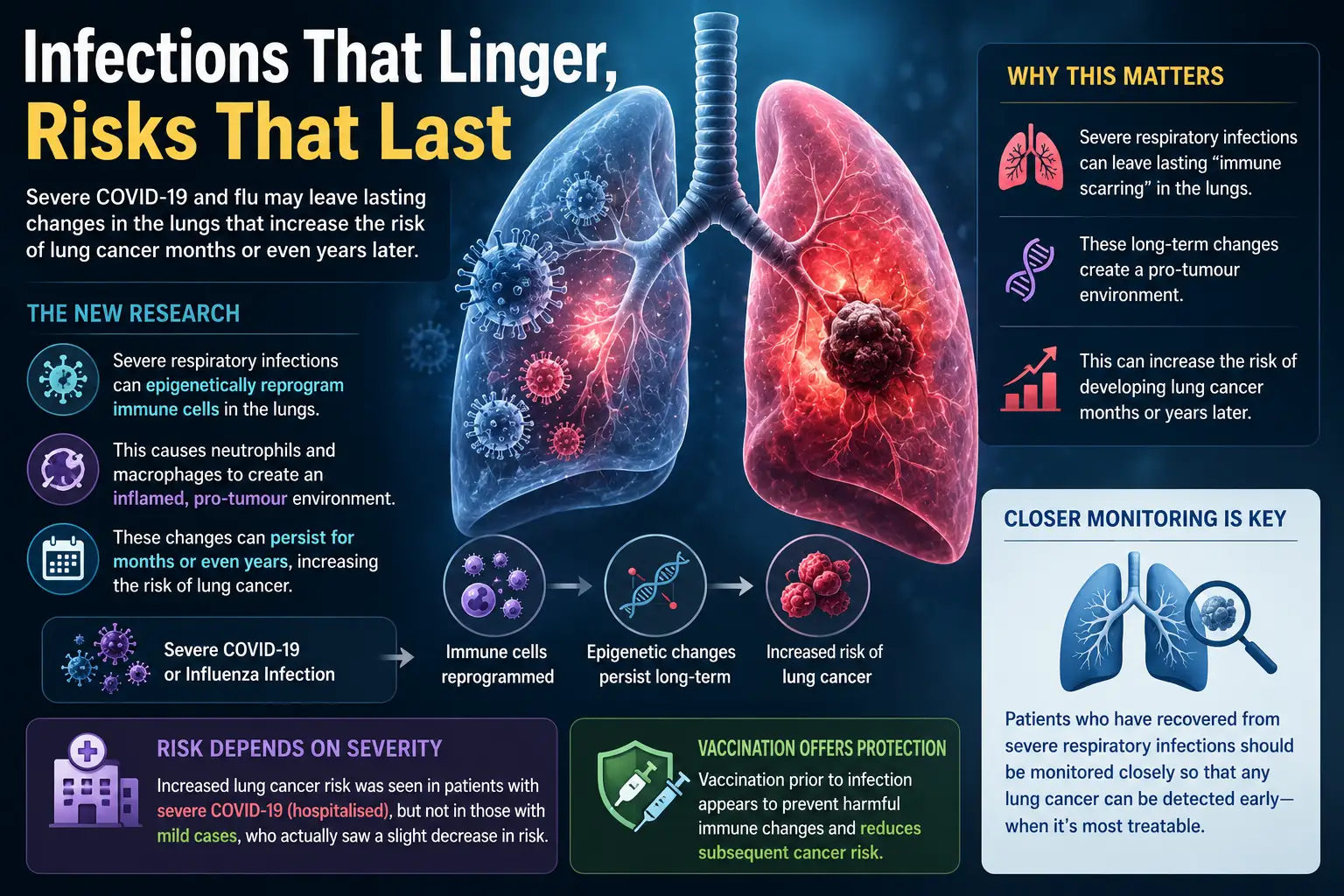
Groundbreaking new research reveals that serious respiratory infections can leave lasting changes in the lungs