Understanding the connection between stroke and sleep.
Home » Stroke and Sleep
Quick links:
The relationship between sleep disorders and stroke is important. Strokes can lead to sleep problems, and some sleep problems can increase the risk of stroke.
Stroke is the second leading cause of death worldwide. Although scientists have uncovered several risk factors for stroke, such as age, diabetes, high blood pressure and atrial fibrillation there are still many cases in which the cause or contributing factors remain unknown.
When you have an apnoea there can be a dramatic drop in blood oxygen (hypoxia). This increases heart rate and blood pressure variability which increases the risk of hypertension and heart arrhythmias.
In addition there is a reduction in blood flow to the brain, further damage to blood vessels, acceleration of atherosclerosis, and increased clotting risk. OSA ultimately increases the risk of fatal and non-fatal stroke between 3-10 fold.
Obstructive sleep apnoea (OSA) is associated with an increased risk of stroke in middle-aged and older adults, especially men, according to new results from a landmark study supported by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health. Researchers from the Sleep Heart Health Study (SHHS) report that the risk of stroke appears in men with mild OSA, and that this risk rises significantly with the severity of OSA. This risk is independent of other risk factors such as weight, high blood pressure, race, smoking, and diabetes.
Conducted in nine medical centres across the United States, the SHHS is the largest and most comprehensive prospective, multi-centre study on the risk of cardiovascular disease and other conditions related to OSA. In the latest report, researchers studied stroke risk in 5,422 participants aged 40 years and older without a history of stroke.
Researchers followed the participants for an average of about nine years. They report that during the study, 193 participants had a stroke — 85 men (of 2,462 men enrolled) and 108 women (out of 2,960 enrolled).
After adjusting for several cardiovascular risk factors, the researchers found that the effect of OSA on stroke risk was stronger in men than in women. In men, a progressive increase in stroke risk was observed as OSA severity increased from mild to severe levels. Our findings provide compelling evidence that OSA is a risk factor for stroke, especially in men. Overall, the increased risk of stroke in men with OSA is comparable to removing 10 years from a man’s age. Importantly, we found that increased stroke risk in men occurs even with relatively mild levels of sleep apnoea.
“Research on the effects of sleep apnoea not only increases our understanding of how lapses of breathing during sleep affects our health and well being, but it can also provide important insight into how cardiovascular problems such as stroke and high blood pressure develop” noted Michael Twery, Director of the NIH National Centre on Sleep Disorders Research in the USA.
There is now abundant evidence that OSA is associated with cardiovascular risk factors and diseases. Research is currently underway to determine how successfully treating OSA can lower a person’s risk of this leading killer.
Successful treatment of hypertension is much less likely if OSA remains untreated. This further accelerates the risk of vascular disease, including repeat strokes.
It is important for your doctor to consider OSA if you have ‘resistant’ hypertension.
In OSA there is night-time hypoxia, lowered cardiac output and reduced cerebral blood flow. This contributes “further noxious stimuli” to a brain already damaged by stroke, which can then become susceptible to further strokes.
Recent studies also found that approximately 70% of stroke patients have OSA, more than 10 times higher than in the otherwise healthy population. Researchers also discovered that the severity of OSA has a direct relationship with functional impairment, and this relationship persisted even after the analysis was controlled for age, weight, and type and location of stroke.
Stroke patients with untreated OSA also have a 40% longer rehabilitation period in hospital. In addition once they left hospital they were still more impaired than the other group. Furthermore, the functional impairment can be relatively refractory to therapy.
Currently, assessment and treatment of OSA are often not part of standard therapy for stroke patients. Based upon this new research Sleep Physicians recommend this be included in the rehabilitation period assessment.
For more information on Stroke click here.
Stay informed with expert tips, research updates, and wellness insights from our team of respiratory and sleep medicine professionals.
Blog of the Week
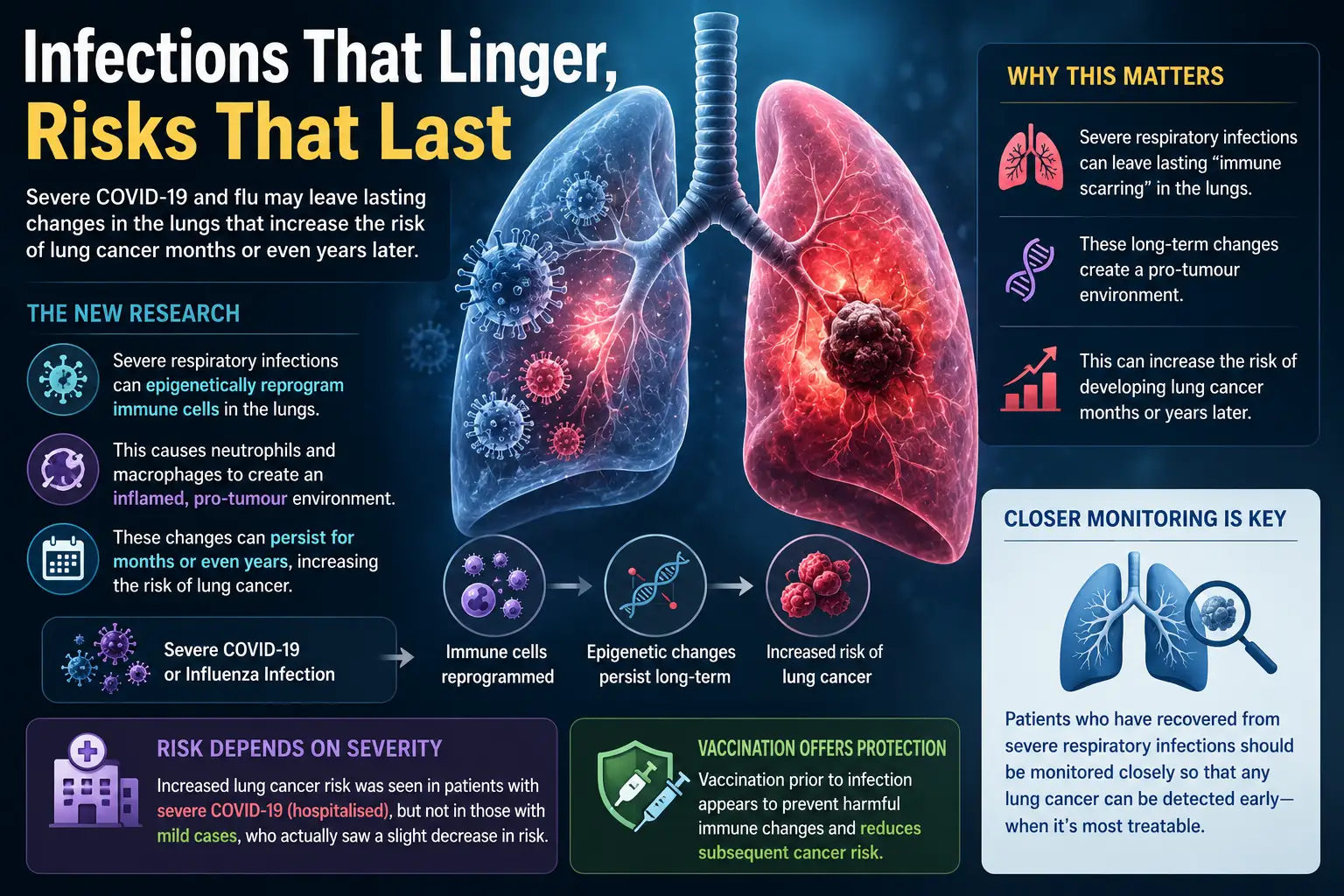
Groundbreaking new research reveals that serious respiratory infections can leave lasting changes in the lungs
Recent

Foods that contain melatonin, tryptophan, certain carbohydrates and magnesium are those that aid sleep, but

Struggling to stay comfortable while using your CPAP machine? The right pillow can make a
Groundbreaking new research reveals that serious respiratory infections can leave lasting changes in the lungs

Millions of people abandon CPAP therapy every year. A repurposed epilepsy drug could offer a