Home » When the Brain Won’t Settle: Mapping the Neural Imbalance Behind Restless Legs Syndrome
Tags
When the Brain Won’t Settle: Mapping the Neural Imbalance Behind Restless Legs Syndrome
Restless legs syndrome (RLS) is often described through symptoms, but this large MRI review helps quantify what is actually different in the brain. Across 49...
Restless legs syndrome (RLS) is often described through symptoms, but this large MRI review helps quantify what is actually different in the brain.
Across 49 studies including more than 1,200 patients, a consistent pattern emerges: changes are modest in size, but repeatable across the same networks.
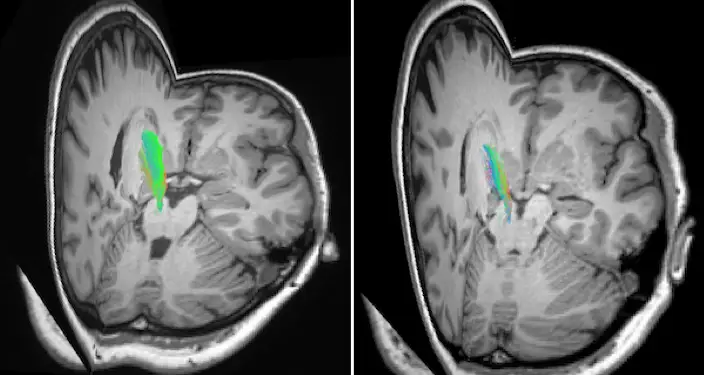
One of the clearest findings relates to brain iron levels. Multiple studies reported significantly reduced iron in the substantia nigra and thalamus, with effect sizes generally in the moderate range. This is clinically meaningful because iron is required for dopamine production. Even moderate reductions can impair how effectively movement is regulated, particularly at rest. This is seen in the sructural changes of the dopamine system through the differences in MRI between the healthy individual (left) and those with RLS (right) below. The nerve bundles (coloured), in a region known to be important for controlling movement, are markedly reduced in the person with RLS.
Functional MRI results show a second consistent pattern. Connectivity within sensory and motor networks is increased, while connectivity in dopaminergic control circuits is reduced. In several studies, these differences reached statistical significance at p < 0.05 in thalamic and sensorimotor regions. For patients, this reflects a measurable imbalance: stronger incoming sensory signals paired with weaker inhibitory control.
Structural changes are present but smaller. Differences in grey matter volume and cortical thickness are typically subtle, often less than 5 to 10 percent, but still statistically significant across groups. These changes are most consistently seen in regions involved in movement and sensation rather than the whole brain.
White matter findings add another layer. Diffusion imaging shows reduced integrity of key connecting pathways, again with moderate effect sizes, indicating less efficient communication between regions rather than complete disruption.
Importantly, several studies also linked these imaging findings directly to symptoms. Higher connectivity in sensory regions and lower iron levels were both associated with greater symptom severity scores, reinforcing that these are not incidental findings but relate to what patients actually feel.
Taken together, the numbers tell a consistent story. The differences in RLS are not dramatic structural abnormalities, but reproducible, moderate shifts in brain chemistry and network activity. Sensory systems are measurably more active, movement-control systems less effective, and the balance between them is altered.
For patients, this helps explain why symptoms feel so specific. The urge to move is not random. It reflects a quantifiable change in how the brain is regulating sensation and movement, particularly during rest when these systems should be quietest.
References:
Pani, T., Mogavero, M. P., Ferri, R., & Lanza, G. (2025). Unraveling the pathophysiology of restless legs syndrome from multimodal MRI techniques: A systematic review. Sleep medicine, 125, 31–56. https://doi.org/10.1016/j.sleep.2024.11.020
Restless legs syndrome (RLS) is often described through symptoms, but this large MRI review helps quantify what is actually different in the brain.
Across 49 studies including more than 1,200 patients, a consistent pattern emerges: changes are modest in size, but repeatable across the same networks.
One of the clearest findings relates to brain iron levels. Multiple studies reported significantly reduced iron in the substantia nigra and thalamus, with effect sizes generally in the moderate range. This is clinically meaningful because iron is required for dopamine production. Even moderate reductions can impair how effectively movement is regulated, particularly at rest. This is seen in the sructural changes of the dopamine system through the differences in MRI between the healthy individual (left) and those with RLS (right) below. The nerve bundles (coloured), in a region known to be important for controlling movement, are markedly reduced in the person with RLS.
Functional MRI results show a second consistent pattern. Connectivity within sensory and motor networks is increased, while connectivity in dopaminergic control circuits is reduced. In several studies, these differences reached statistical significance at p < 0.05 in thalamic and sensorimotor regions. For patients, this reflects a measurable imbalance: stronger incoming sensory signals paired with weaker inhibitory control.
Structural changes are present but smaller. Differences in grey matter volume and cortical thickness are typically subtle, often less than 5 to 10 percent, but still statistically significant across groups. These changes are most consistently seen in regions involved in movement and sensation rather than the whole brain.
White matter findings add another layer. Diffusion imaging shows reduced integrity of key connecting pathways, again with moderate effect sizes, indicating less efficient communication between regions rather than complete disruption.
Importantly, several studies also linked these imaging findings directly to symptoms. Higher connectivity in sensory regions and lower iron levels were both associated with greater symptom severity scores, reinforcing that these are not incidental findings but relate to what patients actually feel.
Taken together, the numbers tell a consistent story. The differences in RLS are not dramatic structural abnormalities, but reproducible, moderate shifts in brain chemistry and network activity. Sensory systems are measurably more active, movement-control systems less effective, and the balance between them is altered.
For patients, this helps explain why symptoms feel so specific. The urge to move is not random. It reflects a quantifiable change in how the brain is regulating sensation and movement, particularly during rest when these systems should be quietest.
References:
Pani, T., Mogavero, M. P., Ferri, R., & Lanza, G. (2025). Unraveling the pathophysiology of restless legs syndrome from multimodal MRI techniques: A systematic review. Sleep medicine, 125, 31–56. https://doi.org/10.1016/j.sleep.2024.11.020