

26 Jul Chronic cough
A systematic approach to diagnosis and treatment remains the most effective way to manage chronic cough. The baseline investigations that should be available in all or almost all patients with persistent cough are a chest radiograph and spirometric tests.
A large portion of cases of chronic cough are caused by the following conditions:
- Asthma, including cough variant asthma
- Chronic Rhinosinusitis
- GORD
- Chronic bronchitis/COPD
- Infections
Which clinical investigations are useful in the diagnosis of chronic cough?
Spirometric and Complex Pulmonary Function testing – assess for obstructive or restrictive patterns, associated with hyperinflation and/or gas trapping, reduction in lung volumes/confirm restrictive pattern, DLCO/KCO impairment, parenchymal lung impairment.
Bronchial Provocation testing – Bronchial challenge (Mannitol) testing can provide important information. Bronchial hyperreactivity and normal spirometric measurements raises the possibility of cough variant asthma
Exhaled Nitric Oxide (FeNO) testing – Exhaled nitric oxide (NO) levels may be lower in non-asthmatic coughers, allowing some differentiation from asthmatic cough. Represents a simpler alternative to induced sputum test. Furthermore, nasal nitric oxide (nNO) may be elevated in patients with paranasal sinus inflammation.
Rhinomanometry – measures nasal airway resistance. Reversible elevated nasal airway resistance may be noted in patients with paranasal sinus inflammation.
Rhinomanometry data showing nasal airway obstruction (left) improving post decongestant (right):
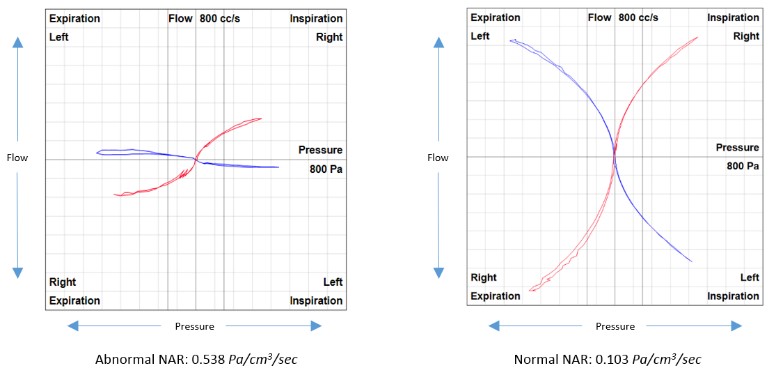
Normal Rhinomanometry: Nasal Airway Resistance (NAR) <0.300 Pa/cm3/sec.
A significant response to decongestant: >30% reduction from baseline NAR.
Chest radiograph, Allergen Testing, Sinus imaging, CT thorax and gastrointestinal investigations may also form part of the diagnostic investigation.