

03 Oct Sleep and pregnancy
Posted at 22:57h
in Medical Newsletter
Pregnancy is accompanied by certain alterations in physiology secondary to hormonal, mechanical, and circulatory changes as a characteristic of pregnancy. A Clinician who examines a pregnant woman for potential sleep-disordered breathing (SDB) should consider the potential implications of these pregnancy adaptations; some changes may predispose patients to SDB.
- Anatomic narrowing and increased resistance within respiratory system during pregnancy. These changes begin early in the first trimester and increase progressively throughout pregnancy. They may lead to a reduction in dimensions of the nasopharynx, oropharynx, and larynx, with consequent increased airflow resistance and an increase in the Mallampati score as pregnancy progresses. (Izci B, Vennelle M, Liston WA, et al. Sleep-disordered breathing and upper airway size in pregnancy and post-partum. Eur Respir J 2006;27(2):321–7.)
- Pien and colleagues studied 105 women (28% normal weight, 24% overweight, and 50% obese). SDB was present in 10.5% of their subjects during the first trimester (median, 12 weeks). By the third trimester (median, 33.6 weeks), 26.7% had SDB. (Pien GW, Pack AI, Jackson N, et al. Risk factors for sleep-disordered breathing in pregnancy. Thorax 2014;69(4):371–7)
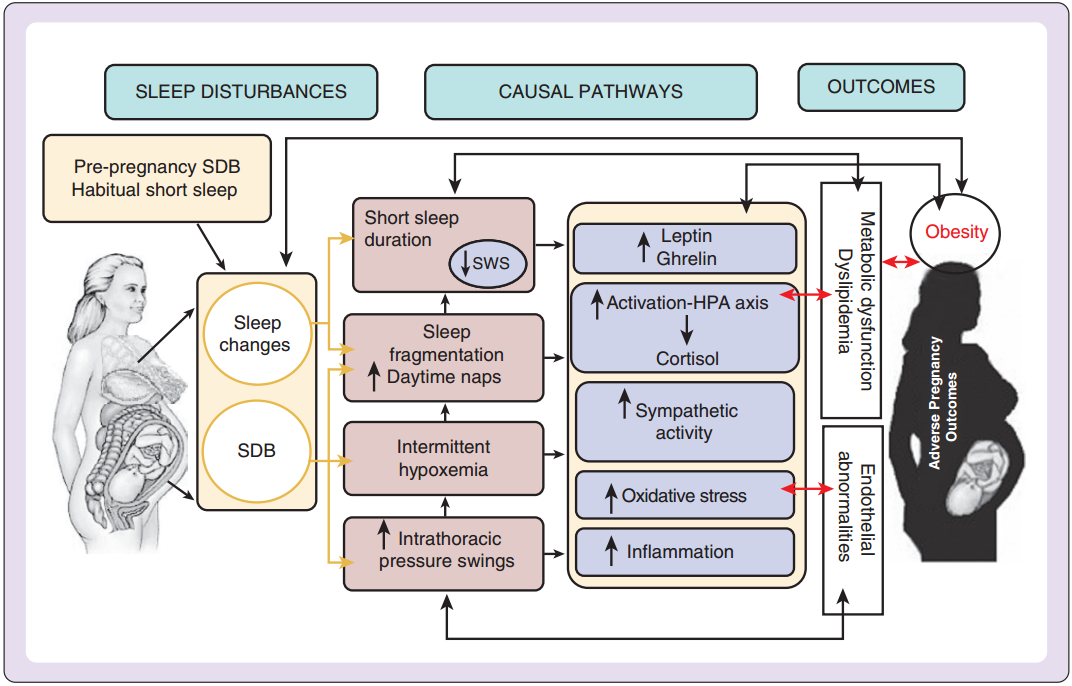
- Facco and associates studied 128 high-risk pregnant women with one or more of the following risk factors: obesity, chronic hypertension, presentational diabetes, previous preeclampsia, and twin pregnancies. See figure 1.
- A systematic review of five observational studies noted that pregnant women with SDB were at increased risk for development of gestational diabetes (adjusted OR, 1.86; 95% CI, 1.30 to 2.42). (Pamidi S, Pinto LM, Marc I, et al. Maternal sleep-disordered breathing and adverse pregnancy outcomes: a systematic review and metaanalysis. Am J Obstet Gynecol 2014;210(1):52.e1–14.)
- Among 55,781,965 women, OSA was associated with increased risk of hospital death (adjusted OR, 5.28), pulmonary embolism (adjusted OR, 4.47), and cardiomyopathy (adjusted OR, 9.01). (Louis JM, Mogos MF, Salemi JL, et al. Obstructive sleep apnea and severe maternal-infant morbidity/mortality in the United States, 1998- 2009. Sleep 2014;37(5):843–9.)
- The potential effects of sleep disordered breathing on the fetus are not well known, however studies point to an increased likelihood of fetal growth restriction among pregnant women with moderate to severe SDB (OR, 1.44; 95% CI, 1.22 to 1.71). (Ding XX, Wu YL, Xu SJ, et al. A systematic review and quantitative assessment of sleep-disordered breathing during pregnancy and perinatal outcomes. Sleep Breath 2014;18(4):703–13.)
- One study found more LGA infants born to women with SDB than to obese and normal-weight control subjects (17% vs. 8% and 2.6%, respectively) (Louis JM, Auckley D, Sokol RJ, Mercer BM. Maternal and neonatal morbidities associated with obstructive sleep apnea complicating pregnancy. Am J Obstet Gynecol 2010;202(3):261.e1–5.)