28 Nov Two Distinct Patterns of Hyperpnea During Cheyne-Stokes Respiration: Implication for Cardiac Function in Patients With Heart Failure
Elisa Perger, MD et al
http://jcsm.aasm.org/viewabstract.aspx?pid=31113
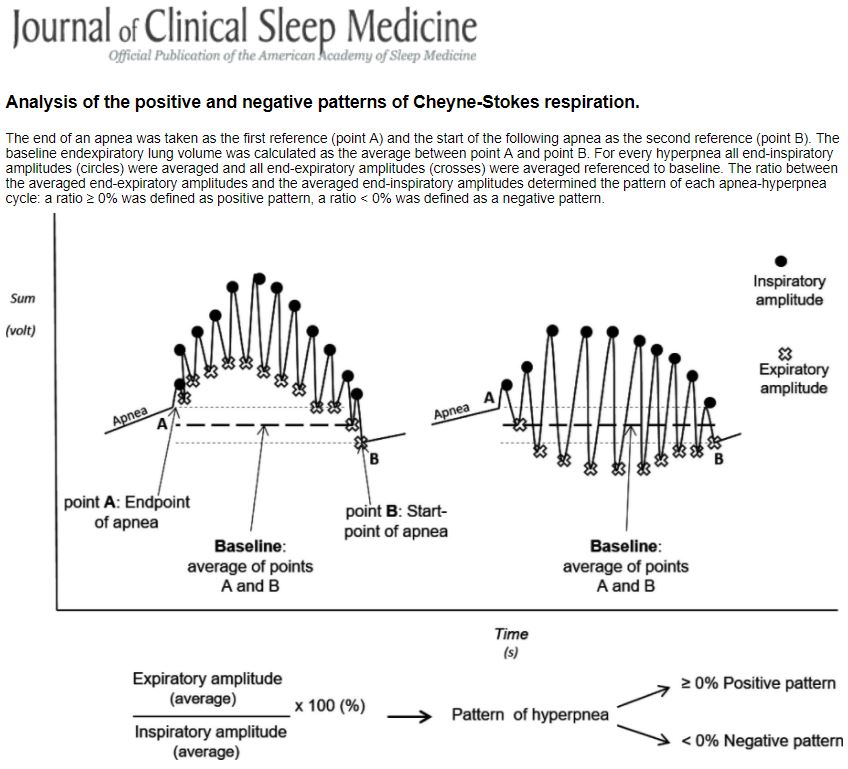
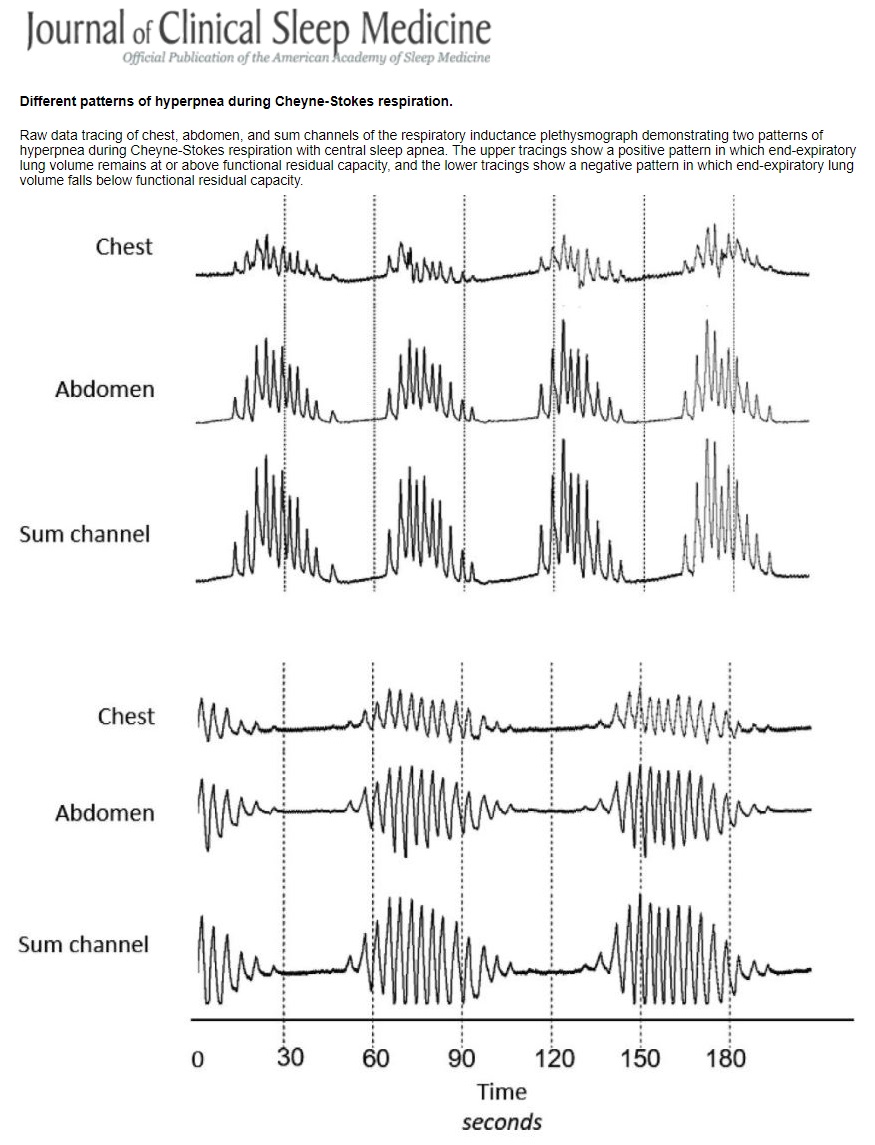
Cheyne-Stokes respiration (CSR) is a breathing pattern observed typically in heart failure (HF) described by a cyclical waxing and waning pattern. This study found two distinct patterns during the hyperpnea phase: a positive pattern where end-expiratory lung volume (EELV) remains at or above functional residual capacity (FRC), and a negative pattern where end-expiratory lung volume falls below FRC.
The negative pattern was found to be associated with more severe HF. These patients had a longer hyperpnea time, longer CSR cycle time (indicating worse cardiac function) and worse New York Heart Association (NYHA) class than those with a positive pattern. Left ventricular ejection fraction (LVEF) and lung to circulation finger time (LFCT) did not differ between groups although stroke volume (SV) and cardiac output (CO) was not directly measured.
Previous studies have shown that treating CSR in heart failure with LVEF <45% had a negative effect on mortality and that CSR may be acting in a protective mechanism in this cohort.
Identifying the negative pattern of hyperpnea in some CSR has offered some discussion as to the mechanisms of action in relation to HF. Firstly, this negative pattern would produce a higher amount of intra-thoracic pressure during expiration by recruiting expiratory muscles to remove air below the FRC. This positive pressure could assist cardiac function during the expiration phase by impeding venous return and reducing right ventricular preload, in turn allowing more complete filling of the left ventricle. Additionally left ventricular afterload would be reduced due to the reduced pressure gradient between the thorax and the intracardiac space caused.
Secondly during CSR, hyperventilation occurs as a response to central apnoeas due to pulmonary congestion and increased chemo-receptor responsiveness. This hyperventilation phase increases the work placed on the inspiratory muscles which may be susceptible to fatigue. It is thought that by recruiting the expiratory muscles during exhalation, the inspiratory muscles may be unloaded somewhat by passive elastic recoil during the first part of inhalation as the chest wall moves outward back to FRC. The persistent activity of the inspiratory muscles throughout expiration can contribute to an increase in EELV. Because EELV fell below FRC during the negative pattern it is very likely that there was less post-inspiratory activation of the inspiratory muscles during the negative than the positive pattern indicating a more compensated CSR pattern in response to chronic and more severe HF.
Some limitations do exist within this study however the observations provide some support for a potential compensatory role of CSR, at least in relation to the negative pattern, in heart failure.